Prior Authorization Automation for Neurology
A practical guide to automating neurology prior authorizations without losing track of therapy evidence, benefit routing, renewals, and human review.
- Last Updated
- June 25, 2026
- Originally Published
- June 25, 2026
- Author
-
 Sohil Bhagat Chief Product Officer, Kairos Health
Sohil Bhagat Chief Product Officer, Kairos Health
This page is part of our PA Automation Complete Guide. Start there for the full workflow; this specialty spoke focuses on neurology, where prior authorization often depends on chronic-therapy evidence, benefit routing, and renewal timing.
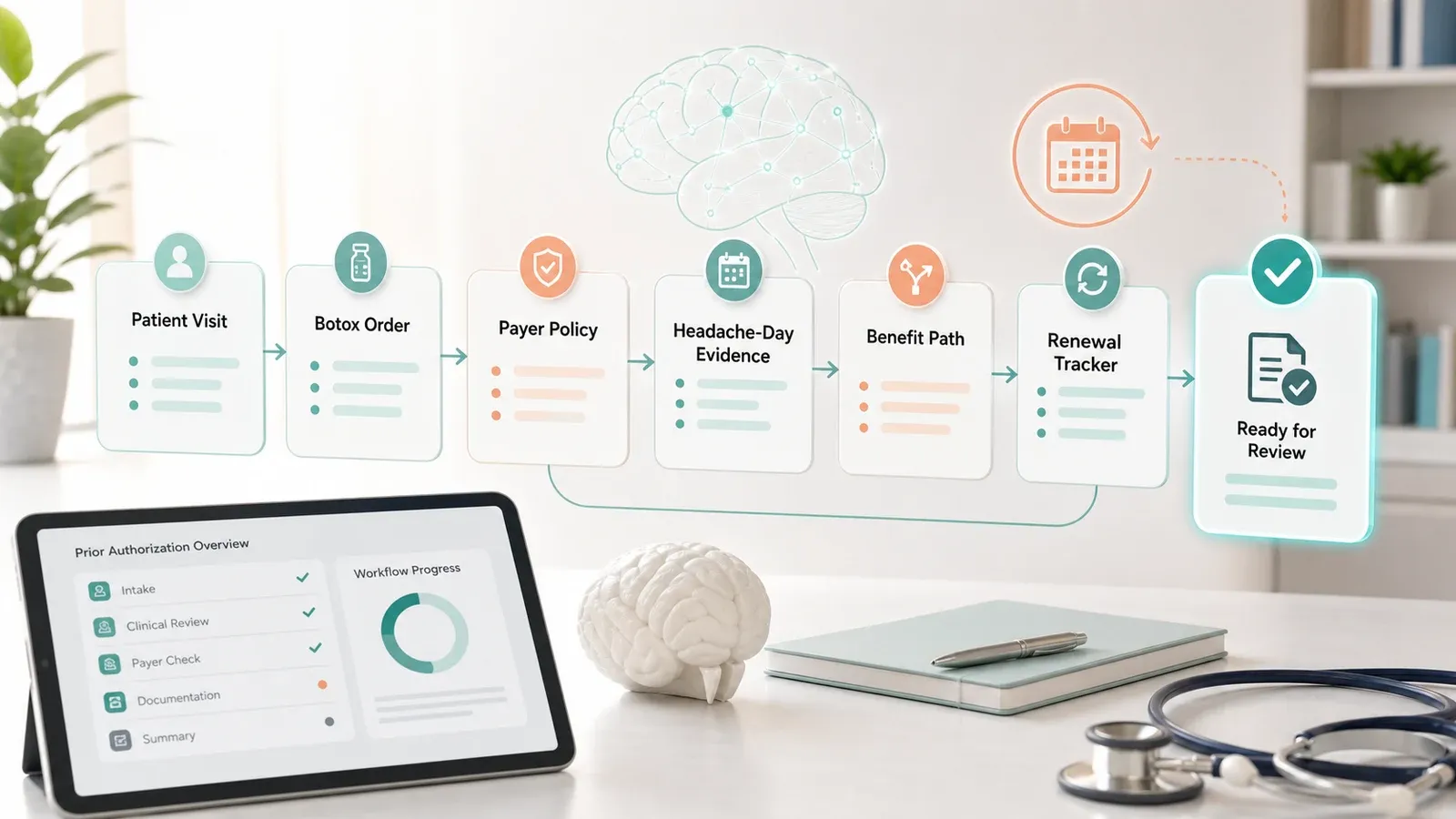
Prior authorization automation for neurology helps practices check whether approval is required, gather clinical evidence, choose the right benefit path, submit through the payer’s channel, and track renewals before the next treatment date. Botox for chronic migraine is a useful example because the PA depends on evidence, routing, and continuity.
Overview
A neurology PA trace should explain why the case is ready, missing evidence, or needs review.
Payer rule
Plan, policy date, initial vs continuation, prescriber, and criteria.
Benefit path
Buy-and-bill, specialty pharmacy, medical benefit, or pharmacy benefit.
Chart evidence
Headache days, duration, prior therapy, dose, interval, and response.
Renewal state
Visits left, expiration date, shipment status, and next action.
Key takeaways
- Neurology PA is renewal-heavy. Chronic migraine, MS infusion, and movement-disorder therapies often need authorization windows, visit counts, and continuation evidence tracked over months.
- Benefit path matters. Botox may run through buy-and-bill medical workflows or specialty pharmacy workflows, and that route changes the operational work.
- Human review still matters. Dose exceptions, unclear headache documentation, denials, peer-to-peer work, and clinical arguments should route to humans with evidence assembled.
Why does neurology prior authorization need specialty-specific automation?
Neurology prior authorization needs specialty-specific automation because payer approval often depends on chronic-disease evidence, medication history, benefit path, and renewal status. A generic form-fill workflow can miss the evidence and timing details that keep a therapy moving.
For Botox chronic migraine, the practice may need to know whether the patient is buy-and-bill or specialty pharmacy, whether the current authorization has remaining visits, whether renewal should start now, and whether the latest note documents headache-day history and prior preventive medications.
Kairos operating observation from neurology workflow discussions: staff often maintain separate trackers for provider schedule, buy-and-bill versus specialty pharmacy, visits remaining, and renewal timing. That is the operational texture a useful automation system has to absorb.
Example: Botox chronic migraine PA trace
In this example, automation has to connect clinical criteria, prior therapy evidence, benefit path, dose and interval, and renewal tracking in one reviewable trace.
The core evidence is clinical. The DailyMed Botox label describes adult chronic migraine using the familiar 15-or-more headache days per month and 4-or-more hours per day threshold, and lists 155 Units with re-treatment every 12 weeks. Payer policies add their own branches. Aetna’s policy includes headache-day criteria and prior preventive therapy requirements. Cigna’s policy includes specialist involvement and continuation documentation. UHC’s policy cites FDA approval, practice guidelines, and trial evidence.
Code fields matter, but they should not take over the article. A CMS billing article for botulinum toxin injections references HCPCS J0585. In the Medicare hospital outpatient PA context, a CMS OPPS list pairs product codes such as J0585 with injection codes such as 64615. That is not a universal Botox PA rule; production software still has to verify coding, site of service, payer, line of business, and current policy.
Botox Chronic Migraine Example
How should automation trace a Botox PA?
A Botox chronic migraine automation trace should start with payer and benefit path, then verify current policy, chronic migraine evidence, prior therapy requirements, dose and interval, and renewal status. Keep the trace readable enough for staff to review.
The automation trace should gather:
- Payer, plan, line of business, benefit path, and policy date.
- Chronic migraine evidence: diagnosis, headache days, duration, and chronicity.
- Prior preventive therapy history, contraindication, or intolerance.
- Dose, units, interval, and prescriber or specialist requirement.
- Initial vs continuation status and documented response when renewing.
- Authorization visits remaining, expiration date, and specialty-pharmacy shipment if relevant.
The output should be a reviewable trace: supported, missing, ambiguous, conflicting, or human review needed. It should not be a black-box approval guess.
What evidence should the chart contain?
The chart should contain the facts the payer asks for, with each answer linked to a source document. For Botox chronic migraine, that usually means diagnosis, headache frequency, duration, prior therapy history, dose, interval, prescriber context, and response for continuation.
For initial requests, payer criteria often ask whether the patient meets chronic migraine definitions and has tried prior preventive therapies. For continuation, criteria usually move toward response, ongoing medical necessity, and timing. Aetna’s policy, for example, separates initial headache criteria from continuation based on maintaining or achieving a reduction in monthly headache frequency. Cigna’s policy similarly asks for documented significant clinical benefit for continuation.
Where do benefit verification and prior authorization connect?
Benefit verification and prior authorization should connect, but they should not be collapsed. Benefits answer whether the plan is active and how the service is covered. PA answers whether the payer approves the requested therapy under its rules.
For Botox, benefit path can decide the operational route. A buy-and-bill case stays closer to the practice’s medical-benefit workflow. A specialty-pharmacy case may require payer or PBM routing, shipment coordination, and confirmation that the drug will arrive before treatment.
Automation should show coverage, date-of-service window, benefit route, policy criteria, submission channel, allowed visits, expiration date, and denial or appeal route together. An authorization can be clinically approved but still fail operationally if the drug does not arrive, the benefit path changed, or the appointment date falls outside the approval window.
Automation Workflow
What should a neurology PA workflow do before submission?
Before submission, neurology PA automation should run a requirement check, evidence check, benefit-path check, and renewal check. Cases with missing or conflicting support should route to human review before staff file.
Check route
Payer, plan, site, benefit path, channel, and policy date.
Map evidence
Diagnosis, headache history, prior therapy, dose, and response.
Check renewal
Visits used, expiration, reference number, and continuation criteria.
Close loop
Decision, visits left, shipment status, write-back, and next task.
A practical deployment can start with a Botox chronic migraine queue. In practice, the most relatable pieces are not exotic clinical rules. They are simple operational facts that drive work: Is this buy-and-bill or specialty pharmacy? How many authorized visits remain? When does the renewal need to start?
| Timing | Automation action | Human review trigger |
|---|---|---|
| Renewal window | Check current authorization, visits remaining, expiration, and benefit path | Expired authorization, changed insurance, unclear route |
| Evidence review | Confirm headache history, prior therapy, dose, and continuation response | Missing evidence, dose exception, or conflicting notes |
| Close-out | Capture decision, reference number, shipment need, and write-back | Denial, more-information request, or peer-to-peer |
CMS’s PA API FAQ is useful context here: even with electronic APIs for non-drug items and services, CMS says the final rule does not require real-time decisions because some reviews still need clinical staff. Neurology drug workflows should be designed for that reality too. Automation should shorten the manual work and surface risk early, not assume every case can be decided instantly.
What should stay human in neurology PA?
Humans should own clinical judgment, dose exceptions, denials, peer-to-peer work, and cases where documentation does not clearly match payer criteria. Automation should assemble the evidence and show the gap.
Keep these cases review-led:
- Requested dose, units, or interval differs from the expected policy pattern.
- The note does not clearly document headache-day criteria or prior preventive therapy.
- A continuation request lacks response evidence or a clean renewal record.
- A denial, reconsideration, or peer-to-peer requires clinical argument.
Buyer Evaluation
How should a neurology practice evaluate PA automation?
A neurology practice should evaluate PA automation on live therapy workflows, not screenshots. The test is whether the system can prevent missed renewals, missing evidence, wrong benefit-path routing, and avoidable treatment disruption.
Useful buyer questions:
| Question | Strong answer | Weak answer |
|---|---|---|
| Can you track Botox renewals by appointment date? | Yes, with visits remaining, expiration, and next task | We show auth status in a queue |
| Can you separate benefits from PA? | Yes, with medical/pharmacy routing and buy-and-bill vs specialty pharmacy | PA approval means the case is done |
| Can you map payer criteria to source evidence? | Yes, each answer cites the note, medication history, policy, or prior auth | The system summarizes the chart |
For the Production Alignment Ramp, start with a narrow set of payer-therapy combinations: Botox chronic migraine by top payers, then MS infusions, then other recurring neurology therapies. Measure renewal timeliness, missing-document rate, staff touches, and days from order to authorization.
Kairos POV
Renewal state is a clinical operations signal. Kairos treats authorization visits remaining, expiration date, benefit path, and continuation evidence as first-class workflow inputs because each one can decide whether treatment proceeds cleanly.
Keep benefit path and medical necessity separate. A Botox case can fail because evidence is missing, because the benefit route changed, or because specialty pharmacy delivery is not ready. Those failures should route differently.
Use source-linked evidence, not free-text confidence. The system should show which note, policy, medication history, prior authorization, or benefit record supports each answer.
Bottom line
Neurology PA automation is not only payer-form completion. For Botox chronic migraine, the workflow has to connect payer policy, headache-day evidence, prior therapy, dose and interval, benefit path, authorization visits, renewal timing, and human-review routing. That is what makes neurology a real specialty spoke under the broader PA automation pillar.
FAQs
What makes neurology prior authorization different?
Neurology PA often combines chronic therapy renewals, diagnosis-specific evidence, benefit-path routing, specialist requirements, and timing. Botox for chronic migraine is a useful example because the workflow tracks headache-day criteria, prior therapy, benefit path, and continuation evidence.
What evidence does Botox PA automation need for chronic migraine?
A Botox chronic migraine workflow commonly checks adult chronic migraine diagnosis, headache-day frequency, headache duration, prior preventive therapy requirements, prescriber specialty, dose and units, treatment interval, and whether the request is initial or continuation.
Does Botox PA automation need both medical and pharmacy benefit checks?
Yes. Botox can move through buy-and-bill medical-benefit workflows or specialty-pharmacy pathways depending on the payer and plan. Automation should keep benefit verification separate from prior authorization while using both to route the case correctly.
Can AI fully automate Botox prior authorization?
AI can help gather chart evidence, compare it with payer criteria, draft portal answers, track renewals, and surface missing documentation. Human review should remain in place for ambiguous notes, dose exceptions, denials, peer-to-peer work, and clinical arguments.
How should a neurology practice evaluate PA automation?
Start with high-volume therapy workflows, then test whether the system can map payer criteria to chart evidence, separate medical and pharmacy benefit routing, track visits and expiration dates, and route exceptions early.